You have no items in your shopping cart.
【Insight】Decoding the Mystery of Nipah Virus's "100 Times Higher Fatality Rate than COVID-19": Tracking the Latest Breakthroughs in "Global Therapeutics and Vaccines"
Recently, the Nipah virus outbreak in West Bengal, India, has rapidly become a global public health concern. According to the latest official report, as of January 26, 2026, the region has cumulatively reported 5 confirmed cases, including 3 nurses, 1 doctor, and 1 healthcare worker—a composition clearly indicating human-to-human transmission within medical institutions.
The high alert surrounding the Nipah virus outbreak stems from two key characteristics:
First, the nosocomial transmission chain is clear: the index case was a patient with respiratory symptoms who died before a confirmed diagnosis, followed by infections among several healthcare workers involved in the treatment.
Second, the Nipah virus maintains a case fatality rate as high as 40%–75%. Compared to SARS-CoV-2 (the original strain had a fatality rate of approximately 1–3%, while Omicron, post-vaccination, is typically below 0.1%), Nipah virus's fatality rate exceeds that of COVID-19 by over 100 times.
Why is this virus named "Nipah" so deadly?
The Nipah virus is not a novel virus. It belongs to the Henipavirus genus, a zoonotic virus with pandemic potential and high lethality, with fruit bats (flying foxes, Pteropodidae) as its natural reservoir.
The Nipah virus can be transmitted to humans through intermediate hosts (such as pigs) or consumption of food contaminated by bats (e.g., raw date palm sap), causing severe acute respiratory syndrome and encephalitis. It has been confirmed to achieve limited but clear human-to-human transmission in close-contact settings, particularly within healthcare facilities and households.
The "high fatality rate" of the Nipah virus is closely related to its "invasion mechanism and potent immune evasion capabilities."
The virus utilizes the Ephrin-B2/B3 proteins, widely expressed on vascular endothelial cells and neurons, as its "receptor," which directly explains its ability to cause systemic vasculitis and encephalitis.
More critically, through a series of viral proteins, it systematically suppresses the host's innate immune responses (especially the interferon system) and inflammatory responses, creating a "stealth" environment conducive to viral replication.
At the molecular mechanism level, the Nipah virus encodes six major proteins,
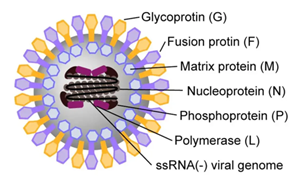
Figure 1: Structure of Henipaviruses (Source: Literature)
.png)
Figure 2: Life Cycle of Henipaviruses (Source: Literature)
The Nipah virus employs multiple viral proteins to inhibit the host's antiviral defenses.
Within the Type I IFN induction pathway, the P protein and its co-translated accessory proteins—V, W, and C—play central roles in immune evasion.
The V protein directly binds to the host viral sensors MDA5 and LGP2, while also inhibiting PP1α/γ phosphatases, thereby preventing MDA5 dephosphorylation and activation.
The W protein primarily localizes to the nucleus, promoting the accumulation of 14-3-3 proteins, which sequester NF-κB subunits and inhibit the transcription of pro-inflammatory cytokines. Additionally, W inhibits TBK1/IKKε-mediated signaling downstream, specifically IRF3 dimerization and nuclear translocation, thereby blocking IFN-I gene induction. Notably, W also impairs TLR3–TRIF-dependent signaling, although the precise molecular mechanisms of this inhibition remain to be fully elucidated.
The C protein is implicated in inhibiting early antiviral IFN responses and the production of pro-inflammatory cytokines.
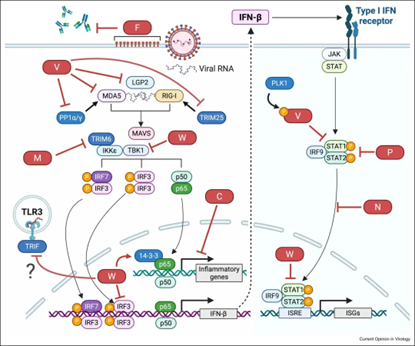
Figure 3: Evasion of Innate Immune Signaling Cascades Mediated by Henipaviruses (Source: Literature)
The M protein targets the E3 ubiquitin ligase TRIM6 for proteasomal degradation, leading to impaired IRF3 phosphorylation and diminished IFN-β induction.
While the F protein is not directly immunosuppressive, it contributes to immune evasion by promoting cell-to-cell viral spread and shielding viral epitopes with N-linked glycans, thereby hindering antibody recognition.
Following interferon activation, a critical phase where cells initiate "Interferon-Stimulated Gene (ISG)" expression to produce antiviral proteins, the Nipah virus N and P proteins directly inhibit ISG transcriptional activation by binding and preventing the signal transducer and activator of transcription factors STAT1 and STAT2 from entering the nucleus.
The V protein, after phosphorylation by PLK1, modulates STAT1 binding affinity and attenuates STAT1/2-mediated signaling.
Furthermore, the nuclear-localized W protein interacts with unphosphorylated STAT1, further suppressing ISG expression.
The attitude towards the Nipah virus should be one of "scientific vigilance, not panic."
Although its fatality rate is high, its transmissibility is limited, and its transmission routes are well-defined. For individuals, strict adherence to preventive measures is the fundamental guarantee of safety.
Currently, there are no officially approved specific therapeutics or vaccines for the Nipah virus.
However, global scientific research has made several positive advancements, bringing hope for future prevention and treatment.
- A study published in November 2025 in Emerging Microbes & Infections demonstrated that the oral nucleoside analog VV116 (a drug already approved for COVID-19 treatment) potently inhibits Nipah virus in both cell and animal models, significantly reducing viral load in infected animals, alleviating lung damage, and markedly increasing survival rates to 66.7%. It is currently a highly promising candidate therapeutic, but it still requires rigorous human clinical trials to confirm its efficacy and safety.
- Research published in November 2025 in npj Vaccines analyzed 27 monoclonal antibodies targeting the Nipah virus (NiV) G protein. The study found that LN1F9 is a standout antibody in animal models, providing 100% protection in both prophylactic and therapeutic settings, capable of directly blocking virus binding to the receptor (ephrin-B2). This study presents the first comprehensive mapping of antigenic sites on the NiV G protein, identifying and validating a key, cross-species conserved vulnerable epitope.
- According to information on the Coalition for Epidemic Preparedness Innovations (CEPI) website, the University of Oxford initiated the world's first Phase II clinical trial for a Nipah virus vaccine candidate in December 2025. This trial is being conducted in Bangladesh, a region with recurrent Nipah outbreaks, through collaboration between Oxford University and the local International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b). It is funded by CEPI and aims to systematically evaluate the safety and immunogenicity of the ChAdOx1 NipahB vaccine in the local population.
Key Research Tools by Biorbyt
The rapid development of the aforementioned drugs and vaccines relies on the support of a series of key research tools. In laboratory research, Nipah virus recombinant proteins (such as G protein, F protein), monoclonal antibodies, and recombinant antibodies are indispensable core reagents. If you need information on Nipah virus or other viral research reagents, please feel free to contact us!
References
- Kim J, Lee SJ, Ahn DG, Yoo JS. Immune evasion and pathogenesis of henipaviruses. Curr Opin Virol. 2026 Jan 21;74:101509. doi: 10.1016/j.coviro.2026.101509. Epub ahead of print. PMID: 41570456.
- Zhang Y, Yao Y, Song S, Gao G, Peng Y, Liu H, Chen M, Zheng W, Tian G, Xie Y, Shen J, Xiao G, Hu T, Shan C, Zhang L. The oral nucleoside drug VV116 is a promising candidate for treating Nipah virus infection. Emerg Microbes Infect. 2025 Dec;14(1):2587983. doi: 10.1080/22221751.2025.2587983. Epub 2025 Nov 19. PMID: 41257471; PMCID: PMC12632212.
- Zhou D, Wang Y, Yao Y, Kuang W, Cheng R, Zhang G, Liu H, Li X, Chiu S, Deng Z, Zhao H. Antigenic landscape of Nipah virus attachment glycoprotein analysis reveals a protective immunodominant epitope across species. NPJ Vaccines. 2025 Nov 28;11(1):5. doi: 10.1038/s41541-025-01319-2. PMID: 41315143; PMCID: PMC12780214.
- https://cepi.net/university-oxford-launches-worlds-first-phase-ii-nipah-virus-vaccine-trial